Choosing a doc/hospital

Hello - My dad has just been diagnosed with esophageal adnocarcinoma with at least one node involved. He's pet scanning today. I am trying to figure out who are the rock star docs for EC. I see anecdotal stories of good experiences at Mayo and MD Anderson and Sloane... But how do you choose where? We live closest to Wash DC where Georgtown U and Hopkins have good reputations. But are they the very most cutting edge? Docs there are involvd in clinical trials, widely published, seem to be cutting edge...But are they the best we can do?
Also can anyone provide advice on learning about chemo drugs - seems the knowledge and drug developments are moving "fast" and I want to make sure we're headed in that direction.
Your advice gratefully accepted...
Comments
-
Dr. James D. Luketich @ University of Pittsburgh Med. Ctr. YES
Greetings “Daddyshelper”
Am glad you wrote here. Even though we wish your daddy had never had this diagnosis, he certainly needs a “helper.” And by your letter, I take it that you want him to have the very best. So here’s the recommendation of an Esophageal Cancer Patient (Adenocarcinoma at the GE Junction) (EC T3N1M0)! We are “still tickin’” into our 14th year of survival with no recurrence.
You will probably receive more than one name and it will most likely be from a “satisfied patient.” Being 77 years old myself, I remember some slogans that stood out above all the rest. I think these are descriptive of the onset of Esophageal Cancer, the Ivor Lewis Minimally Invasive Esophagectomy (MIE) and one fantastic Thoracic surgeon, Dr. James D. Luketich at University of Pittsburgh Medical Center.
MORTON’S SALT - When it rains, it pours.... HALLMARK cards ~ When you care enough to send the very best!... ZENITH TV – The quality goes in before the name goes on!... COCA COLA –“ It’s the Real Thing” & “Things go better with Coca Cola”... TIMEX WATCHES – “It takes a lickin’ and keeps on ticking!
So let’s just be honest. We Esophageal Cancer patients (and caregivers) know what it’s like to “take a lickin’” and “keep on tickin’!”
In 2002, my husband was then 65 years old. William worked for Ford for 42 years before retiring in January of 2002. In November of that same year, he was diagnosed with Adenocarcinoma at the GastroEsophageal (GE) junction. Official diagnosis (EC T3N1M0). This meant that all four walls of his Esophagus and 2 lymph nodes were found to contain cancer. It all began with a pesky hiccup that persisted for 2 months or so before I insisted my husband go see a doctor.
So we went to our GP, who in turn set up an appointment with a Gastroenterologist. Within 2 days an Endoscopy was performed. We went home not knowing when to expect a report on the results. At that time we didn’t know what an Endoscopy was or even how to spell it. But we were quick learners, when the phone rang the next day about 2:30 PM in the afternoon. The call went like this. I answered the phone. My husband was sitting beside me at his computer. So the phone rings and the voice I hear is the Gastroenterologist. “Hello Mrs. Marshall. This is Dr. Ryan. I do wish you had stayed around yesterday. I needed to talk with you. Your husband has CANCER!”
No I didn’t lose consciousness, but I must admit I was shocked! Cancer from a hiccup??? Dr. Ryan began to use words I had never heard before, like “Esophageal” and “Squamous”. I asked, “How do you spell it?” And from that day to this we have never stopped learning about Esophageal Cancer.
We went back to our GP, Dr. Acra, who was an internist himself and had been our family doctor for over 30 years. He placed a call to Dr. Ryan while we were there. We sat in his office and listened to Dr. Acra. He asked, “Are you sure you have the right William Marshall?” The answer was, “YES!” Dr. Acra had tears in his eyes, and it brings tears to my eyes, as I recount that day and many that followed.
Talk about “takin’ a lickin’”…we didn’t know what each day would bring. All of a sudden, our calendar filled up with appointments with people whom we had never met who dealt with specialties we had never heard of. But we were soon to learn. I will say that we never entered the “state of denial.” We readily accepted the diagnosis based on the expertise of the doctors involved.
Dr. Ryan and Dr. Acra agreed that the best Thoracic surgeon was Dr. Hubbard, and indeed he was excellent and caring. Dr. Hubbard told us we needed to see an “oncologist”. He said, “I’m going to send you to the “doctors’ doctor.” His name would be Dr. Paul Conkling.
Now this is where we hit a “bit of a snag!” We said to ourselves, mind you were knew nothing but that we equated “chemotherapy” with almost instant death. Little did we know that it would turn out to be a life saver. But we balked for a time, thinking “oh who wants to go through that? We’ll just have the surgery and forget about having chemotherapy!” But God intervened, and gave us the good sense to cooperate with Dr. Hubbard’s insistence that we at least go talk with the oncologist. And so not to appear uncooperative with the surgeon, we agreed to go.
I asked questions about how long people had lived with this diagnosis. Dr. Conkling never “pushed us” but answered all our questions. Now mind you, we were dealing with late stage EC. We were still “uneducated” as to the whole subject of Esophageal Cancer at the time. Life suddenly became a whirlwind of decisions we needed to make when we were least prepared to make them! Actually, we were praying about where to go and what to do, yet still feeling uncertain if we were making the right choices. God didn’t print out a list of instructions to be followed in chronological order. Wouldn’t that be nice? But I did have a notepad and pencil and asked many questions. Then with our trusty computer, we found out “more than we ever wanted to know.”
And so I want to share the ultimate destination—that being the University of Pittsburgh Medical Center…and the most gifted, intelligent, and caring Thoracic surgeon for anyone that has been diagnosed with Esophageal Cancer, DR. JAMES D. LUKETICH, pioneer of the Ivor Lewis Minimally Invasive Esophagectomy aka MIE.
As talented as Dr. Hubbard was, he was only trained to perform the TransThoracic Esophagectomy (TTE) which involves 2 massive incisions and a lot longer recuperative period, plus more open to infection and a higher morbidity rate. It wasn’t until after all pre-op treatments had been completed, and my husband was about 10 days away from surgery, that my sister-in-law from Florida sent me an e-mail regarding a Dr. Luketich who was lecturing a group of physicians there. He was speaking about the latest laparoscopic procedure for Esophageal Cancer. He is a renown Thoracic surgeon known world-wide.
From that we placed a call to a Dr. Luketich. He did NOT require any special referrals from other doctors. He simply said, “Bring us all your records. We will perform our own examination, and if you’re a good candidate for this type of operation, we will gladly perform the surgery.” Needless to say, they “worked us in quickly”. We traveled by car up there and “flew home on the wings of an angel.” We were so excited about the new surgery as opposed to the oldest. Now many surgeons have performed the Ivor Lewis Minimally Invasive Esophagectomy, but it requires 2 massive incisions. It was first introduced by a Dr. Ivor Lewis, hence the name Ivor Lewis, yet it was anything but minimally invasive.
UPMC is a teaching hospital, and doctors go there to update their skills, or learn the new techniques relative to EC, as well as other types of surgery. The MIE is performed in other countries now as well as here in the United States. And talk about “cutting edge”, there is the Hillman Cancer Center there equipped with the latest technologies. I don’t know any place that surpasses UPMC. They are known all over for organ transplants as well.
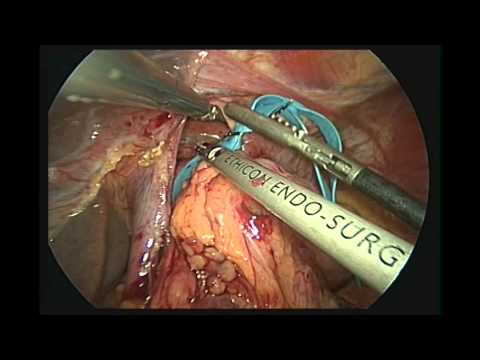
In the mid-1990s, Dr. Luketich pioneered a totally laparoscopic surgery for Esophageal Cancer patients. It was still considered in its infancy when my husband had his surgery there May 17, 2003. His MIE Surgery consisted of 7 Band-Aid size cuts (Incisions just large enough to insert the necessary instruments to perform the surgery. Now at that time William had one incision on the upper left side of his neck in the area of his collar bone. It was just a bit larger than the rest, because this is where the cancerous Esophagus was removed. But now, Dr. Luketich has made even further improvements. (Fine tuning if you will). He now makes that incision further down on the right side of the chest. In doing so, the Pharyngeal and Laryngeal nerves are not disturbed. They are more subject to damage with a neck incision than with a chest incision.
However, I see that this has been improved upon as well. According to https://web.duke.edu/surgery/2013_Thoracic_Masters/session5_ivor_lewis_luketich.pdf there are now only 5 openings for the MIE surgery. There are four 5-mm ports (that = 5/32 of an inch) and one 10-mm port (That = 25/64 of an inch). The 10-mm opening is in the lower right side of the chest where the diseased Esophagus is removed.
My husband was in the hospital a total of 5 days. He was in ICU for one day—put in a step-down unit on Day 2—placed on the regular EC ward on Day 3—passed the swallow test on Day 4—Discharged on Day 5—downtown shopping with me on Day 8.
This was my husband’s treatment schedule:
Week 1 ~ (02-10-03) Chemo 96-hr. continual infusion of Carboplatin/5-FU
-
Weeks 2, 3, and 4 ~ (02-17-03) 5-day-a-week radiation treatment.
-
Week 5 ~ Combination radiation plus SECOND chemo continuous 96-hr. infusion
-
Week 6 ~ (03-17-03) Final week of radiation.
-
Repeat PET Scan on 04-28-03 ~ results - COMPLETE ERADICATION OF TUMOR in Esophagus and the 2 affected lymph nodes
-
Ivor Lewis Minimally Invasive Esophagectomy, May 17, 2003 by Dr. James D. Luketich @ UPMC
I took pictures all along the way and have photos of him downtown Pittsburgh. During the next 3 months we toured parts of Maryland, West Virginia as well as Pennsylvania. We returned to UPMC at regularly-scheduled intervals for the follow-up visits that were necessary.
From Washington, DC to Pittsburgh, PA, the distance is 244 miles. It will take you about 5 hours by automobile. (Faster of course if you take a plane.)
We couldn’t be more pleased and more proud of Dr. Luketich. He is one of God’s gift to the world of medicine! Incidentally, one distinction in choosing a good Thoracic Surgeon is to review his biography and see how many publications they have written that were published in medical journals. Dr. Luketich has written hundreds! And always choose a hospital that majors in the type of surgery needed by you. At UPMC the MIE is the surgery of choice. It is their standard operating procedure, unless for some reason the patient has a unique problem that warrants the “OPEN” surgery.
We know of none finer. My husband really did “take a lickin’ and he’s still tickin’”. May it be so with “your daddy” as well!
Wishing you and daddy all the best,
Loretta Marshall, Wife of William, EC T3N1M0—MIE surgery @ UPMC on May 17, 2003 by Dr. James D. Luketich.
Helpful references:
1. http://news.cancerconnect.com/types-of-cancer/esophageal-cancer/
Good reference for EC - This is an excellent pdf file on CANCER OF THE ESOPHAGUS.
2. http://www.cancer.org/acs/groups/cid/documents/webcontent/003098-pdf.pdf
A “pdf” excellent source of information in great detail outlining diagnosis, tests, stages, surgery, etc.
3. http://www.chemocare.com/chemotherapy/drug-info/default.aspx
An all-inclusive list of chemotherapy drugs, plus their side effects (Our preferred source for learning about any given drug.
4. http://www.mirm.pitt.edu/our-people/faculty-staff-bios/james-d-luketich-md/
Biographical notes on Dr. Luketich
5. http://www.ncbi.nlm.nih.gov/pubmed/?term=Luketich+JD[Author]
(List of 349 publications by Dr. James D. Luketich)
6. http://www.vitals.com/doctors/Dr_James_Luketich/profile
Web link where patients can check credentials
7. http://www.healthgrades.com/physician/dr-james-luketich-32n79
8. http://www.upmc.com/Video/Pages/default.aspx?vcat=937;#3753ef4c-73b8-4be7-b0c7-9c5fd91b952c|Lung+and+Thoracic+Surgery
Video by Dr. Inderpal Sakaria talking about treatment at UPMC for MIE procedures (He is now located elsewhere but he trained under Dr. Luketich at the time of this video) - Note there are 2 Short Videos by Dr. James D. Luketich – one for Esophagectomies and one for treating GERD
“Esophageal Cancer: Surgical Innovations - James D. Luketich, MD, highlights advances in esophageal cancer treatment through innovative surgery. The UPMC Esophageal and Lung Surgery Institute is a leader in developing novel surgical approaches to minimize recovery time and scarring while maximizing results and quality of life for patients after surgery. “
9. http://www.upmc.com/Video/Pages/default.aspx?vcat=937;#3753ef4c-73b8-4be7-b0c7-9c5fd91b952c|Lung+and+Thoracic+Surgery
10.
 https://www.youtube.com/watch?v=hx4hS21AbuI&feature=related
https://www.youtube.com/watch?v=hx4hS21AbuI&feature=relatedThis is one of the best surgeons on the West Coast. Initially Dr. Nguyen worked with Dr. Luketich in the 90s when the MIE was in its infancy. Anyone closer to California would do well to seek out the services of this Thoracic Surgeon.
Uploaded on May 4, 2011- DUE TO THE GRAPHIC NATURE OF THIS VIDEO, VIEWER DISCRETION IS ADVISED. - Minimally Invasive Esophagectomy featuring Ninh T. Nguyen, MD, Professor of Surgery Chief, Division of Gastrointestinal Surgery, University of California, Irvine Medical Center (SDMK13CD0800259)
11.
 https://www.youtube.com/watch?v=u3o30epRTiM
https://www.youtube.com/watch?v=u3o30epRTiMLecture to physicians from Dr. Nguyen detailing Minimally Invasive Esophagectomy
12.
https://www.youtube.com/watch?v=u3o30epRTiM" Published on Jul 18, 2013 - A sample clip of minimally invasive esophagectomy, taken from the Video Atlas of Advanced Minimally Invasive Surgery (CT Frantzides & MA Carlson, editors; Elsevier, 2013), an operative atlas consisting of (1) a textbook with color illustrations and (2) narrated DVD video summarizing each procedure. The procedure in this sample clip was performed by James D. Luketich, Lawrence Crist, and Benny Weksler. The full video is copyrighted 2013 by Elsevier."
13.
 https://www.youtube.com/watch?v=QxiDzHkwyLA
https://www.youtube.com/watch?v=QxiDzHkwyLAMinimally Invasive Esophagectomy - Dr. Dawn Jaroszewski - Lecture on benefits of MIE over other types of Esophagectomies
0 -
-
Update - A separate post-script to "Daddyshelper"
Wednesday - May 4, 2016 - This is an "update" on my "update". Yesterday was simply disastrous. I could not get the letter past the "SECURITY ERROR" notice that constantly popped up. Then by some magic, it finally went through, but had multiple lines between each paragraph. But this Wednesday morning, I tried one more time to "EDIT" the page and put the text out there as it should be. And lo and behold, it posted as it should have yesterday. I sure hope the site "gets this ERROR notification" fixed when there is nothing wrong with the information being submitted.
----------------------------
(My first note on Tuesday 5-3-16 read - Please forgive the way this letter posted. It was not the way I "submitted" it. But somehow it got through. I pulled up the ltr to "edit" it and remove some of the lines, but the "ERROR" message came up once more. I tried sending you a private msg. as well, and an "ERROR" msg. came up again, so if this gets through, guess it's a fluke. But anyway, I'm glad it posted.)
Loretta
0 -
Best Wishes
Hello,
One of the first things I emphasize to folks just starting down this road is that EC is not a minor issue where convenience is a paramount issue in deciding your course of treatment. This is not an issue to be dealt with at your local hospital, unless you happen to live down the street from MSK or Hopkins. You seem to be doing well by trying to identifying top of the line places to go for treatment. I'm not going to specify a great doctor (although my own oncologist is a "rock star" in my mind) because that would just be anecdotal evidence based on my own, singular positive experience. I'm certain she's also had patients who have died as have all oncologists. I think you are doing right to try to find centers that specialize and excel in treatment of EC. This isn't a sprained ankle to be treated at the nearest ER. My current treatment is weekly chemo that I've been doing for 4 1/2 years. Every week I drive directly past the front door of four large hospitals on my way to the hospital that I feel is best for me. This hospital had the best combination of medical oncologists, radiation oncologists and surgeons that was managably close to my home (I am fortunate to live in an area with several world class cancer centers).
While I don't want to steer you towards anything other than what your research leads you to believe is your best option, I will say that if you consider Hopkins to be a viable option for you geographically, you are at least starting off your search quite well.
Hope everything works out well for your father,
Ed
0 -
Joined this group to help my brother
Hello everyone,
My brother was just diagnosed with esophageal carcinoma (biopsy came back yesterday). I stayed up until 2a.m. reading this site and found some very helpful information .... as well as caring people. At this point I don't know what stage or which type of cancer cells he has . He is in the hospital and the Drs are meeting with him today . He is at Eastern Maine Medical Center and I am on Long Island,NY. I am trying to locate the best team of doctors to treat him. I see that EMMC has not seen many cases of this cancer though the information is from 2010. I am looking for links to doctor and hospital ratings as well as input from this group. My head is spinning ! He and I have been the primary care givers to our 92 yr old Mom who is living with me and has vascular dementia. His slogan was always 'No man down' and now I want to help him as much as possible. Thanks for listening and being here.
0 -
"rjollie"~U R smart 2 help your brother~EMMC not best for EC !rjollie said:Joined this group to help my brother
Hello everyone,
My brother was just diagnosed with esophageal carcinoma (biopsy came back yesterday). I stayed up until 2a.m. reading this site and found some very helpful information .... as well as caring people. At this point I don't know what stage or which type of cancer cells he has . He is in the hospital and the Drs are meeting with him today . He is at Eastern Maine Medical Center and I am on Long Island,NY. I am trying to locate the best team of doctors to treat him. I see that EMMC has not seen many cases of this cancer though the information is from 2010. I am looking for links to doctor and hospital ratings as well as input from this group. My head is spinning ! He and I have been the primary care givers to our 92 yr old Mom who is living with me and has vascular dementia. His slogan was always 'No man down' and now I want to help him as much as possible. Thanks for listening and being here.
A very early good morning to you “rjollie”
Am I glad you wrote? You bet! As always we are never happy to hear of another case of Esophageal Cancer. However, those of us who have progressed further “along the Esophageal road” can think a bit more clearly than you at this moment. Confusion is normal at this point, and “sorrow” doesn’t have to be defined. You will find patients that are ready to share their experiences with you. Furthermore, there is a special FACEBOOK group that includes many Esophageal Cancer patients. I know of many on that site, but my husband and I simply do not post on FB or Twitter. It’s not an “exclusive” club because they welcome newcomers, but as a group they are FREE to share their experiences, and comment as they please without fear of one special moderator critiquing their speech and telling them what they can and cannot say! Political correctness is run amuck these days. Any and everything we say will be challenged by someone in this world. I’ve jokingly said that I should start a new small business. It would consist of small foam rubber chips the size that could be worn on the outside of one’s clothing, and always on the shoulder. So people could have their main offense listed there, and you would then know not to “violate their space!” Now there certainly would be a lot of people who need to “wear a chip” because I’ve never seen so many people “offended” these days. What I say is they need to deal with a real problem—take CANCER for instance. That’ll get your “feet on the ground” and a lot of petty things will pale by comparison from that moment on. We on this site are grappling with reality and “life and death” situations. And I’m sure that I can vouch for everyone on this site when I say we do a 180° turn when we see our name at the top of a medical report with a cancer diagnosis. Suddenly one’s life plans are turned upside down, and priorities are rearranged. I chuckle when someone complains about small things. I sometimes say, “Try cancer on for size.” Well you get my drift. Okay that’s my pet peeve. Now back to your letter. You are seeking advice about the best places to find help for your brother, and I always recommend Dr. Luketich because he is the one who “saved our lives.” We give God the ultimate credit, but He gifts people with special abilities who are “smarter than the average guy!” And that’s the kind of doctor you want for your brother.
Often I am not familiar with the medical facility where a person is receiving treatment. When they tell me, I then key in the name of that hospital, and see where they rank, and in what specialties. I also research the biography of any doctor that they mention. There is always a biographical sketch on each hospital link that tells about the training of their medical team.
Another way I look check up on a doctor who is trained to perform the Minimally Invasive Esophagectomy is this—I key in the name of the surgeon, and then I put Minimally Invasive Esophagectomy at the end. If that person’s name comes up and it is included along with the MIE word, then I know that this particular surgeon has been involved in some way with the newest type of surgery.
If I can’t find out a great deal from the Internet, I call the hospital itself, and ask for the Thoracic Surgery department. I then speak with some knowledgeable person in that department and ask what surgical procedure their surgeons are trained to perform. If there is more than one surgeon in the department, I ask specifically which ones have been trained to perform the MIE. I also want to know HOW MANY ESOPHAGECTOMIES they personally perform in a year. He should perform at least 25 or so to qualify as experienced in my opinion.
All surgeons in all medical hospitals have not necessarily upgraded their skills to include the latest surgery, although they may possess a wealth of experience in the earlier forms of an Esophagectomy. The oldest being the Transthoracic Esophagectomy – TTE for short – also referred to as OPEN surgery or simply “Ivor Lewis Esophagectomy” – so named after Dr. Ivor Lewis who first pioneered an Esophagectomy back in the mid-1940s.
It will require the longest period of recuperation. Granted the surgeon may be excellent in his field, but your brother will be the one to be “cut on” and your brother is the one that will have to recuperate from the surgery itself. There is less morbidity, less blood loss, shorter hospital stays, and a quicker return to a normal state of health, with the laparoscopic surgery than one who has to recuperate from 2 massive incisions. That’s understandable. So if there’s a better way to remove the diseased Esophagus, why not pursue that method?
Another Esophageal surgery is called the “Transhiatal Esophagectomy” – THE for short. This method is less invasive than the OPEN surgery, but still has larger incisions than the Ivor Lewis Minimally Invasive surgery. Dr. Mark Orringer from the University of Michigan improved on the older Ivor Lewis procedure. He made his mark in the mid-1970s.
Then along came Dr. James D. Luketich who pioneered the least invasive procedure in the mid-1990s. It is called the Ivor Lewis Minimally Invasive Esophagectomy – MIE for short. That is our preference.
So I’m glad you wrote quickly to see what info you could find out about the best hospital for your brother. I have checked out EEMC, and you will want to move your brother away from that facility asap based on their ranking in my opinion. Obviously they are NOT equipped to handle a major surgery like Esophageal Cancer. Now I can rank no one higher than Dr. James D. Luketich, who is the pioneer of the latest totally laparoscopic procedure for Esophageal Cancer. The larger the hospital, and the volume of Esophagectomies performed at their facility, makes a world of difference in how well the patient fares. Hospitals which only perform a few Esophagectomies a year, cannot be compared to one which specializes in a high volume of Esophagectomies and ones that are more difficult at that. The University of Pittsburgh Medical Center has a well-earned reputation for performing Esophagectomies. The Minimally Invasive procedure is their regular modus operandi now.
So I will just say, brace yourself for a rough ride, but I admire your attitude in “not leaving your brother behind.” Moreover, having overseen the care of my mother when she was in her late 90s, I applaud you for taking on yet “another patient.” I am sending you our e-mail address and phone # by private message. We should not ever give out our personal information on the public link here. If you ever want to call and talk to my husband, he would be delighted to answer your questions.
We’ve been conversing with EC patients now since my own husband had his MIE @ UPMC on May 17, 2003. Actually he was diagnosed in late 2002, and had pre-op chemo of Carboplatin and 5-FU here at home. He then had the MIE procedure on May 17th, a day that will forever remain in our memory. We started down a new road that day. It was like a second honeymoon, because I certainly had “mixed emotions” as I watched the orderly wheel my husband out of site. From there I sat in the “waiting room”, which I often refer to in my own situation, as “God’s waiting room.” I never knew if I would see him alive again. This is an extremely serious surgery. Most do come out alive, but there have been some that didn’t make it, and I already knew that much. So, we vowed that if we “lived through” this Stage III diagnosis, we would try to help inform as many people as possible about the best places and the best doctors, depending on the patient’s ability to travel and of course what their insurance policy dictates! My husband attends a support group here locally for Esophageal Cancer patients each month, and is a source of inspiration for all the newbies. He is the “longest survivor” in the group.
My first piece of advice is to have a 2nd Opinion ASAP. And make that appointment with a qualified medical facility and a highly-trained Thoracic Surgeon that has a great reputation for treating Esophageal Cancer patients. I know that Dr. Luketich has a reputation for accepting patients that are difficult cases. As far as I can determine, he doesn’t require any special referral from another physician. We simply called up and made our own appointment.
Moreover, he is good at “fixing other surgeon’s mistakes” as well. For instance if the new “gastric tube” is slightly twisted when it is transformed into a new Esophagus, the patient can have difficulty swallowing. So you don’t want any “do-overs” for your brother. One surgery is enough. And then after the surgery, there will be a readjustment to the way your brother’s body will function. For one thing, he will sleep in an elevated position, his meals will be many “mini” meals rather than big helpings at one time. And all that takes time. And his recuperative period will be greatly shortened by the laparoscopic method if he chooses the MIE. And that choice should be yours to make.
If all goes well, and there is no residual cancer in any of the lymph nodes removed for pathology during the surgical procedure, he will not require post-op chemo. Clinical trials have shown that patients diagnosed with EC fare best with a tri-modal approach—that being preferably chemo and radiation prior to an Esophagectomy. If the chemo is given at the beginning of treatments it will be called “neo-adjuvant” chemo. If there is any more chemo prescribed “after” the surgery due to residual cancer in any of the nodes tested, it will be necessary to do some “clean-up” chemo after surgery, and that will be called “adjuvant” therapy. And that’s another advantage of the MIE. The patient will be able to start that adjuvant chemo much sooner because his recuperative period will be much shorter. (This is always contingent upon the health of the patient post surgery, of course.) Chemo for most is a “draining” process and fatigue is one constant companion.
Okay this is just to say hello, and to let you know that if there is anything you want to ask about, please write again. I’m not the only one monitoring this post obviously. There are new patients just beginning treatments, while others are due to undergo surgery soon, and others have come through the surgery, and have “lived to tell about it.”
I will say that after my husband had his 2nd opinion @ UPMC, they corresponded with our oncologist here locally. UPMC and VA Oncology kept in close touch. My husband had already completed his pre-op work-up here locally. He then traveled to UPMC for the actual MIE surgery on May 17, 2003. Thank God there was no residual cancer found in any of the 22 lymph nodes examined for residual cancer, so no post-op chemo was recommended. Radiation is given in order to shrink the tumor. Chemo is given which circulates throughout the body in the process of killing as many tumors as possible. So keep us posted. Let us know what the recommendations of this medical team are. Definitely you will want to move on and get that much needed 2nd opinion. But you will want to decide first where that will be. If the ability to travel is limited, or the insurance coverage dictates how many places your brother can go, that will play a part in your decision.
But we have often called Dr. Luketich and said, “Do you have a surgeon in this particular area that you would recommend that has been trained to perform the laparoscopic surgery? He will give me the names of only those whom he deems experienced enough, or else he will not recommend them. He doesn’t operate on the “good old buddy system.”
Below my name are web links to EEMC that speaks for itself. And by the way, keep a record of what doctors your brother has seen, what services were given him at the time, and ask for a copy of their findings as soon as they are available. When we go to the doctor, we ask for a copy of the treatment report. You will want to ask for a copy of all the records and scans and reports to pass onto the next team. They may tell you to get them from the “Medical Records Department but you should start that “collection” now, so you will have a complete list of treatments received thus far and for what.
The doctors will also want to perform their own tests in addition to reviewing the information from the first group of doctors there at EEMC. But your brother needs to move on asap. Moreover, in a medical situation of this type, many hospitals I know will require that the patient fill out a form with the names of those he allows to speak with the doctors on your behalf. No nurse is required to tell you anything if your name isn’t on the list, so be sure to tell your brother if any medical doctor, or facility requires he fill out a form similar to that, that you want your name to be included. That’s important.
Okay, “rjollie”, this list below my name will keep you up again till the wee hours of the morning, but I’m up, so you may as well be. Late tonight, I cooked up about 10# of pork BBQ, and I am late in answering you, although I read your letter a bit earlier. You know some of us women still “cook from scratch”, and I’m one of them. My idea of a restful moment would be to sit out back on the patio in a rocking chair and browse through a good country cookbook, while the birds are singing and wind chimes are ringing. That’s relaxing to me. Well enough of me. You can read more of my story if you click on the picture of my husband, William and me. Some people don’t enter any additional info on that page, but I always check it when writing to a patient. It’s helpful to know “about” them if possible.
With that I will say “good night” or rather “good morning”.
Loretta Marshall, wife of William Marshall, diagnosed with Adenocarcinoma at the Gastroesophageal (GE) junction in 2002. (EC Stage III (T3N1M0) – MIE surgery at UPMC on May 17, 2003 and now into 14th year of survival with presently no evidence of disease (NED)!
______________________________________________________
Please just refer to my posting to “daddyshelper” when they asked about where to find the very best surgeons specializing in Esophageal Cancer. So every bit of info will be helpful to your brother as well. I am always long-winded in my responses. I shall never forget the absolute shock at hearing that my husband had Esophageal cancer. After I asked the Gastroenterologist how to spell it, we made it our business to know all we could about it. We don’t know everything, and of course anything you read here is best discussed with your brother’s medical team, but we aren’t in the habit of giving out bogus info. Yet all the postings here emanate from our own personal experience. And that’s why this discussion link exists. None of us are in the business of diagnosing patients but helping them along the way.
__________________________________________________
Here are some suggestions for researching hospitals and doctors. First I will list EEMC ad you can decide for yourself if you think your brother will find the best treatment there. If “no man down” is your brother’s motto, then EEMC doesn’t fit that description. Incidentally, I am often blunt and to the point. But I think you will agree. So I asked “Dr. Google” about the credentials at EEMC. I chose this link and it told me all I needed to know.
2. http://health.usnews.com/best-hospitals/area/me/eastern-maine-medical-center-6110050
3. http://health.usnews.com/best-hospitals/area/me/eastern-maine-medical-center-6110050/cancer
Eastern Maine Medical Center - Cancer Scorecard - Overall Score - 30.7 / 100 - Reputation with specialists – NONE
I keyed in EEMC and selected a page that gave “rankings” for hospitals based on their specialties. So it appears that there is no one qualified to perform an Esophagectomy on your brother here……For gastric cancers, they rank 36.5 out of a possible 100!—“MOVING ON” would you not say?
I say you need look no further here. They have an abundance of nurses. They may do well with radiation services, but that’s not your brother’s primary need. Although pre-op recommendations are chemo/radiation. But that will be determined by the Endoscopic Ultrasound that your brother will have. They seem to have an abundance of nurses for the size of the hospital. And Geriatrics (older folks) seem rank high in their admissions. Frankly, I don’t know how much of a “work-up” you want your brother to have their since they do not specialize in Esophageal Cancer. A basic finding of cancer as a result of an Endoscopy is only the beginning of the tests required to determine the exact stage of the cancer. Then the treatment plan will be determined by the stage of the cancer.
_____________________________________________________________
4. http://health.usnews.com/best-hospitals/area/me/eastern-maine-medical-center-6110050/gastroenterology-and-gi-surgery
You will be interested to know that for the years, 2013, 2014, and 2015 no gastroenterologist or other physicians recommended EMMC as a place to go for difficult problems dealing with any type of gastric cancer, the category under which Esophageal Cancer would fall. So I think this confirms your inclination that your brother needs to seek expert treatment because this is a major cancer, and requires expert care!
____________________________________________________
You wanted to know how to search out the names of surgeons and find out which hospitals major in performing Esophagectomies. I will list some ways I research doctors and procedures on the web, and compare doctors. Here are a couple of sites. One is called Vitals.com. Here is the link for that website.
5. http://www.vitals.com/?gclid=CNShhsvY2MwCFUEkhgod8JoPbw
From there you can choose by the specialty, condition, topic or name. Once you know the name of the doctor you want to check on, you can see his level of education, plus patient reviews for any given doctor, and usually types of insurance he/she accepts and addresses of hospitals and locations where they practice. I always want to see how many medical articles the doctor has had a part in writing that have been accepted by reputable medical journals. For instance, at last posting on Vitals.com, Dr. Luketich had over 340. I also look at the topic that is being written about and see how many of them pertain to Esophageal Cancer in particular.
____________________________________________________
Here is another link to find the best hospitals for cancer.
6. http://health.usnews.com/best-hospitals/rankings/cancer
7. http://health.usnews.com/best-hospitals/area/pa/upmc-university-of-pittsburgh-medical-center-6230029/gastroenterology-and-gi-surgery
Underneath this USNews link of hospital rankings, I chose UPMC. You can access it for information. UPMC was highly recommended by a majority of specialists as hospital among the BEST FOR TREATING VERY CHALLENGING PATIENTS. So you can choose your specialty and see the rankings by category.
____________________________________________________
8. http://www.healthgrades.com/
9. http://www.healthgrades.com/find-a-doctor
This is another link comparable to Vitals.com for checking on a physician’s credentials.
________________________End of references_______________________
0 -
Need to help my daughter and her husband
My son-in-law was just diagnosed with EC that has spread to his liver. He is 38 years old and we are stunned with this diagnosis. They will not perform surgery on the esophagus and are starting chemo. Has appt with radiation specilist in a week. As you most likely know his prognosis is not good. My daughter can not accept this and is asking for help in finding the best treatment for him. We are not giving into this but are trying to get any information we can. We live in southwest Virginia but are willing to travel anywhere to give him a chance. Any advice, information you can provide would help so much. We just don't know where to turn. Thanks for giving your time to this site just knowing there are people willing to listen and help means so much
0 -
Son-in-lawpamelaann5543 said:Need to help my daughter and her husband
My son-in-law was just diagnosed with EC that has spread to his liver. He is 38 years old and we are stunned with this diagnosis. They will not perform surgery on the esophagus and are starting chemo. Has appt with radiation specilist in a week. As you most likely know his prognosis is not good. My daughter can not accept this and is asking for help in finding the best treatment for him. We are not giving into this but are trying to get any information we can. We live in southwest Virginia but are willing to travel anywhere to give him a chance. Any advice, information you can provide would help so much. We just don't know where to turn. Thanks for giving your time to this site just knowing there are people willing to listen and help means so much
Hello Pamelaann,
Sorry to hear about your son-in-law's diagnosis. Surgery is generally not an option when the cancer is stage IV. Radiation is also not a common option because, like surgery, it is targeted to a specific area while stage IV means that the cancer is on the loose. My 2nd time with EC was stage IV (lung) and surgery and radiation were not options for me. I was told chemo was all that could be done, because it is a system wide treatment, and that I would be eligible for a clinical trial to hopefully help. I would view it as a very good sign that radiation may be an option for your SIL.
Just a couple of months before this, herceptin was approved for metastatic EC and GE junction cancer for patients who were HER2+. Fortunately I was at a top of the line cancer center and they knew to test for this. There are still places that forget or don't bother testing. I would strongly recommend that you insist on your SIL getting tested to find out if he is HER2+. The difference it made for me was extraordinary. I was given a prognosis of 7-8 months, but I had a great response to the treatment and am still testing clean almost 5 years later.
Other than finding out your SIL's HER2 NEU status I would suggest the most important thing you can do is to find a high quality cancer center for treatment. This is no minor issue to be handled by the local hospital. A quality hospital will have the latest clinical trials available for your SIL to participate in. He is young and hopefully otherwise strong and as such has the best possible chance of fighting this off. A top shelf hospital will increase his chances.
You mention that your daughter can not accept his prognosis. To the extent that that means she wants to fight, that is great. But if it means she is not able to deal with the whole thing, your SIL is going to need help and support. I've been on four different chemo regimens and by far the roughest was for the metastatic recurrence. By the time I was completing the chemo, everyone who knew me was convinced I was going to die and soon. Turned out the chemo was working wonderfully and it was the side effects that had me seeming near death. But there's no way I could have gotten through without a lot of help and support from others. And I'm the best case scenerio. Work with your daughter to make sure your SIL has folks that he can lean on, because he's going to need it.
Lastly I want to mention that it is perfectly fine to look for a second opinion. I go to a world class cancer center and my oncologist is first rate (she was just named to Biden's "moonshot" panel) but I still went to Hopkins for a 2nd opinion because I didn't like the 7-8 month prognosis. Hopkins told me that the best thing I could do was go back to my hospital because they were recommending the best possible course of treatment for me. But then, at least I knew and was sure of what I was doing.
Well, I wish you guys well on your journey. Please post questions here as you go along. There's probably someone here who's gone through something similar, no matter how odd it might seem to you.
All the Best,
Ed
0 -
Son-In -Laws
Ed, thanks so much for the information. Since this is very new for us I am not sure if his center tested for HER+2. However I will pass this along to them to insist he be tested. After reading your response I have started researching top rated centers. i get that this is defiantly not a condition we want to treat at the community hospitaL I am hoping we can find a top center within easy traveling distance But we will do what needs to be done for his best option
My daughter is a fighter, she took a little time to adjust to all of this and then put all of the family in action. I am retired so research is one of my task.
0 -
Son-in-law
Hi Ed, I hit submit before I had finished. I was reading the ranking sites posted by LorettaMarshall and wondering if this is a good place to research top facilities. Do you have any recommendations for researching the best centers? Since we are close to Maryland Hopkins had already made it on my list.
Again thanks for your time and detail in your response. i am sure many other questions will come up and I am so glad to have the support.
0 -
Son-in-lawpamelaann5543 said:Son-in-law
Hi Ed, I hit submit before I had finished. I was reading the ranking sites posted by LorettaMarshall and wondering if this is a good place to research top facilities. Do you have any recommendations for researching the best centers? Since we are close to Maryland Hopkins had already made it on my list.
Again thanks for your time and detail in your response. i am sure many other questions will come up and I am so glad to have the support.
Hello,
Loretta's suggestion would be a very good place to get started. She's an excellent researcher, and I'd suggest using her as a resource. One of the things I would look for in a hospital is that it is NCI accredited. That designation goes to places that have the most experience and they are most likely to be offering the current clinical trials. I'm not sure what hospitals are close enough to be managable for you, but if Hopkins is geographically possible for you guys, then you're starting off well with your list.
Hope you find a great center close to you,
Ed
0 -
Son-in-law
then I am on the right track. I will review again Loretta's sites. Thanks Ed
0 -
Pamellaann5543~Note info below~I answered U on a separate linepamelaann5543 said:Son-in-law
then I am on the right track. I will review again Loretta's sites. Thanks Ed
Dearest Pamela Ann:
I’ve taken the liberty of creating a new topic line for my answers to your letter here on the Esophageal Cancer forum. That way in the future, if you will come back to this particular subject line, and ask another question, it will be in chronological order. Often we have three or more different patients asking questions on the same subject line. It makes it easier for me to keep up with those that I have previously written to.
http://csn.cancer.org/node/303304
My Original separate post to you can be read here:
___________________________________________
http://csn.cancer.org/comment/1545272#comment-1545272
Here is Part 2. It is posted directly underneath my original. The article simply would not post in its entirety under the first letter to you. Some days the post just goes “zip” and other days I get a notice that says the page is BLOCKED. If I’ve written to Security once, I’ve written 20 times. They’ve tried to help, but so far there are still “kinks” in the system. So here it is. Please keep the two parts together. The second part contains all the web references that will be of great help to you.
As always any of us who monitor this site welcome your questions, and if we can help you find an answer, we will.
Sincere best wishes for your entire family,
Loretta Marshall (William Marshall’s wife) EC Stage III (T3N1M0) He had pre-op chemo and radiation, and then Dr. James D. Luketich performed an Ivor Lewis Minimally Invasive Esophagectomy @ the University of Pittsburgh Medical Center, May 17, 2003 and is still in remission as of this date. Thank God.
0




Discussion Boards
- All Discussion Boards
- 6 CSN Information
- 6 Welcome to CSN
- 122.1K Cancer specific
- 2.8K Anal Cancer
- 448 Bladder Cancer
- 309 Bone Cancers
- 1.6K Brain Cancer
- 28.5K Breast Cancer
- 398 Childhood Cancers
- 27.9K Colorectal Cancer
- 4.6K Esophageal Cancer
- 1.2K Gynecological Cancers (other than ovarian and uterine)
- 13K Head and Neck Cancer
- 6.4K Kidney Cancer
- 673 Leukemia
- 795 Liver Cancer
- 4.1K Lung Cancer
- 5.1K Lymphoma (Hodgkin and Non-Hodgkin)
- 239 Multiple Myeloma
- 7.2K Ovarian Cancer
- 65 Pancreatic Cancer
- 490 Peritoneal Cancer
- 5.5K Prostate Cancer
- 1.2K Rare and Other Cancers
- 543 Sarcoma
- 738 Skin Cancer
- 658 Stomach Cancer
- 192 Testicular Cancer
- 1.5K Thyroid Cancer
- 5.9K Uterine/Endometrial Cancer
- 6.3K Lifestyle Discussion Boards