The Cancer Survivors Network (CSN) is a peer support community for cancer patients, survivors, caregivers, families, and friends! CSN is a safe place to connect with others who share your interests and experiences.
Update on 2010 diagnosis and treatment

In 2010 at the age of 59, I had Da Vinci surgery with a Gleason 4+5=9 and PSA of 9. Post surgical biopsy showed all margins clear with no seminal vesicle involvement and Gleason post-op score was changed to a 4+3=7. Subsequent PSA was non-detectable as tested every three months for the first two years. Five years after surgery I started TRT. (Testosterone replacement therapy)
PSA remained non-detectable with no incontinence and an active sex life. In 2019 the cancer suddenly went active again with PSA rising from zero to 2.0 in 18 months. Auxium PET scan revealed two lesions in my seminal vesicles so I started Lupron with Cassodex for six months. After four months, I had 35 Proton treatments targeting seminal vesicles and prostate bed. A few months later when the Lupron wore off, and my testosterone rose, my PSA started rising immediately. A new PSMA scan at UCLA June of 2020 revealed a microscopic lesion in right pelvic bone.
Three treatments of SBRT was used 6/20/2020 without ADT because doctors said it would not be needed on such a small lesion. But right after SBRT treatment my PSA continued to rise monthly from .29 to 4.9 over six months. (It was a slow rise at first but the last two months my PSA skyrocketed from.68 to 4.9). No one could account for the dramatic rise except that during that time I had a severe eColi blood infection treated with IV antibiotics.
New PSMA scan 10/18/2021 indicated two small lesions in my lower spine and one in my hip bone. So I started ADT 10/27/2021 with three treatments of SBRT performed at UCLA 18 days later. Bloodwork on the day before SBRT showed my PSA had dropped to .070 along with testosterone to almost zero in 17 days. PSA 05/05/2022 was .008 and testosterone <7 ng/dL.
Even after SBRT, we realized that spinal mets means the possibility of lingering rogue cancer cells or micro tumors too small to see on PSMA scans. We hoped that those could be starved with ADT. Dr. Steinberg at UCLA thought that SBRT plus ADT was sufficient. My City of Hope oncologist, Dr. Dorf, continued indefinite Orgovyx with 90-day shots of Xgeva. (My hemoglobin immediately dropped to 12.) At the thirteenth month on Orgovyx, PSA began a slow rise indicating castrate resistance.
We briefly added 250mg Zytiga + 5mg prednisone before starting Eclipse trial (LU-177 I&T) in June 2023. Beginning PSA was 3.3 and directly before fourth injection in August, PSA dropped to .25 Unfortunately, after fourth injection PSA was .30 and rising. It should be noted that due to cardiovascular problems I stopped all ADT right before last LU-177 injection and remain off.
After October PSMA scan, Dr. Kishan at UCLA found two of three original small spine lesions remained and then immediately hit them with one SBRT treatment.
Directly after SBRT I started and completed Provenge series. A month later PSA went from 2.0 to 1.77 and currently remains at 1.7 .
Hemoglobin fluctuates between 9 and 10.6, probably due to the Plutonium LU-177 injections damaging bone marrow. In an attempt to jump start red cell production on 12/27/23 I received an iron infusion which helped a little. Will my bone marrow ever start working again?
I’m not sure if the the SBRT will continue to affect PSA causing it to become non detectable or if it stays the same. We know that Provenge does not affect PSA, yet any PSA level means cancer is somewhere. Plan is for a durable remission with the help of a hematologist overseeing bloodwork and advising how to fortify my immune system.
Special notes:
I tolerated the ADT side effects well with no depression or anxiety, although sometimes I experience brief afternoon fatigue and of course those pesky hot-flashes. I lift weights and hike daily along with wrestling practice twice a week. There has been no weight gain and I am very fit but endurance is declining along with muscle mass. Getting up 4 times a night to pee is aggravating.
I’m learning to play the piano to help reduce the ADT “Brain fog” and this really seems to help along with yoga and meditation.
December of 2021 I had two lengthy laser kidney stone procedures. Apparently left ureter remained clogged with fragments before being discovered 6 months later—which caused the left kidney failure and drop in EGFR to 36. Also had hernia mesh installation via Da Vinci 3/25/2022.
ADT drugs are listed as having potential cardiovascular side effects. A month after starting Orgovyx I began passing out when hiking or lifting weights. The first time I wound up in the ER unconscious, but after three days of testing, the doctors could find nothing wrong.
Eventually a Nuclear CT scan revealed a calcium score of 890. Under heavy exertion my blood pressure occasionally dropped to 77/42 then I either went unconscious, or remained semi conscious until able to lay flat. After laying flat for an hour or two I felt fine again.
Yet Angiogram showed clean arteries. Baffled doctors recommended 4,000mg salt daily to raise blood pressure—and this solved the problem. However after a month of the salt tabs also causing excessive foot swelling I tapered off to one packet of electrolytes daily. So far no more symptoms. Maybe this is due to no longer being on ADT?
Comments
-
Wow, SV,
What a story. You are a great fighter.
You have thrown at it the "mother of all treatments" and managed to survive. The bandit seems to be on the canvas. Thought still young (64), you need a rest.
How about visiting this corner of the Europe in your bike. You would enjoy the local red wines. I could guide you.
Best wishes in your continuing journey.
VG
-
Sorry to read about all the problems you faced over the last ten years or so. And a big thanks for your very informative post; you have seen it all with respect to prostate cancer therapies, that's for sure. Moreover, you encountered additional medical issues that required serious measures.
I do have a minor question, if you don't mind. Why the TRT five years after the surgery; was your T low all along?
-
You've had quite a PCa journey to date, SV. My hat is off to you for your remarkable fight against the bandit. I wish you the best of outcomes moving forward.
Most important, we have not heard you complain one time about your situation, or dwell on the 'woe is me' aspects of your PCa journey. You are a true soldier, in my book, and I wish that other folks will take note of your journey and recognize their relatively good fortunes on their PCa journeys.
Keep fighting!!
-
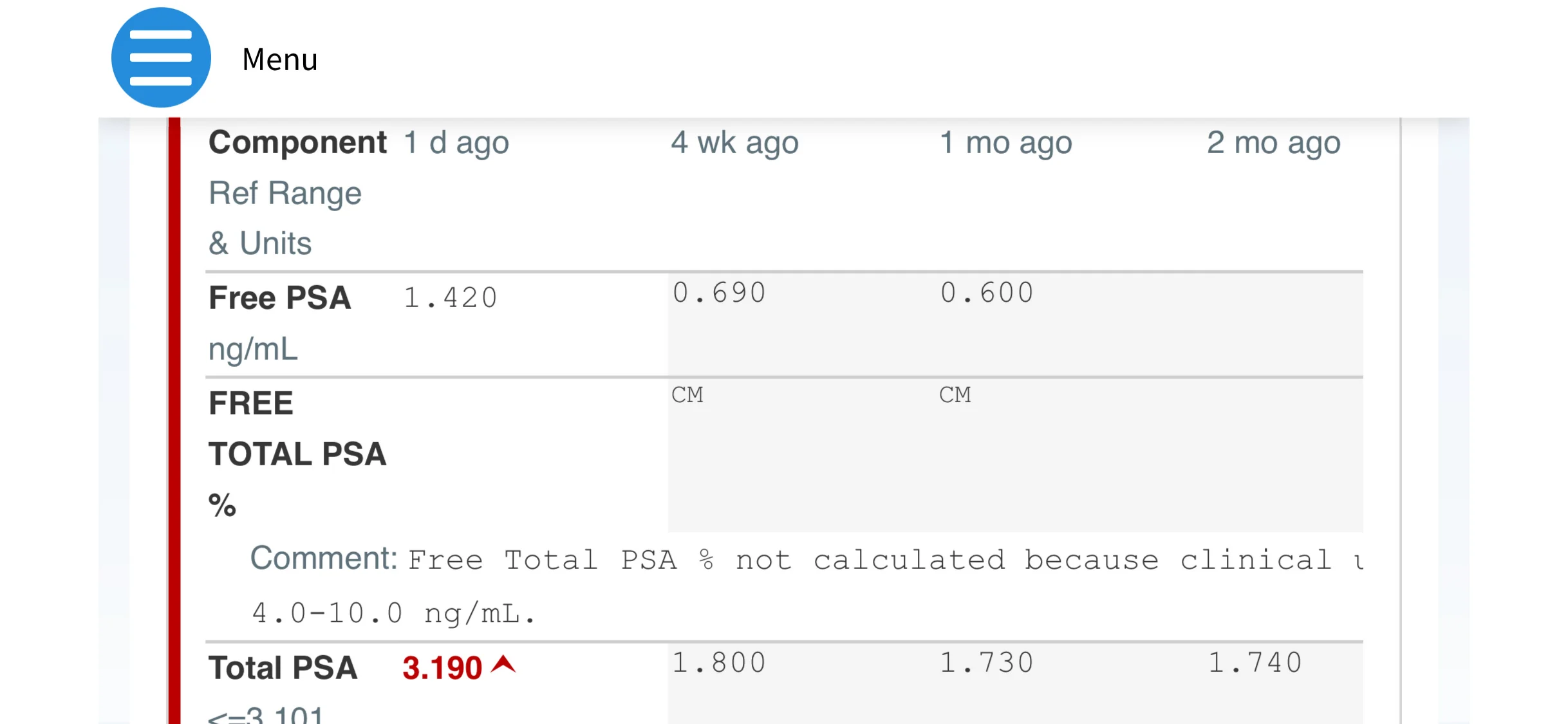
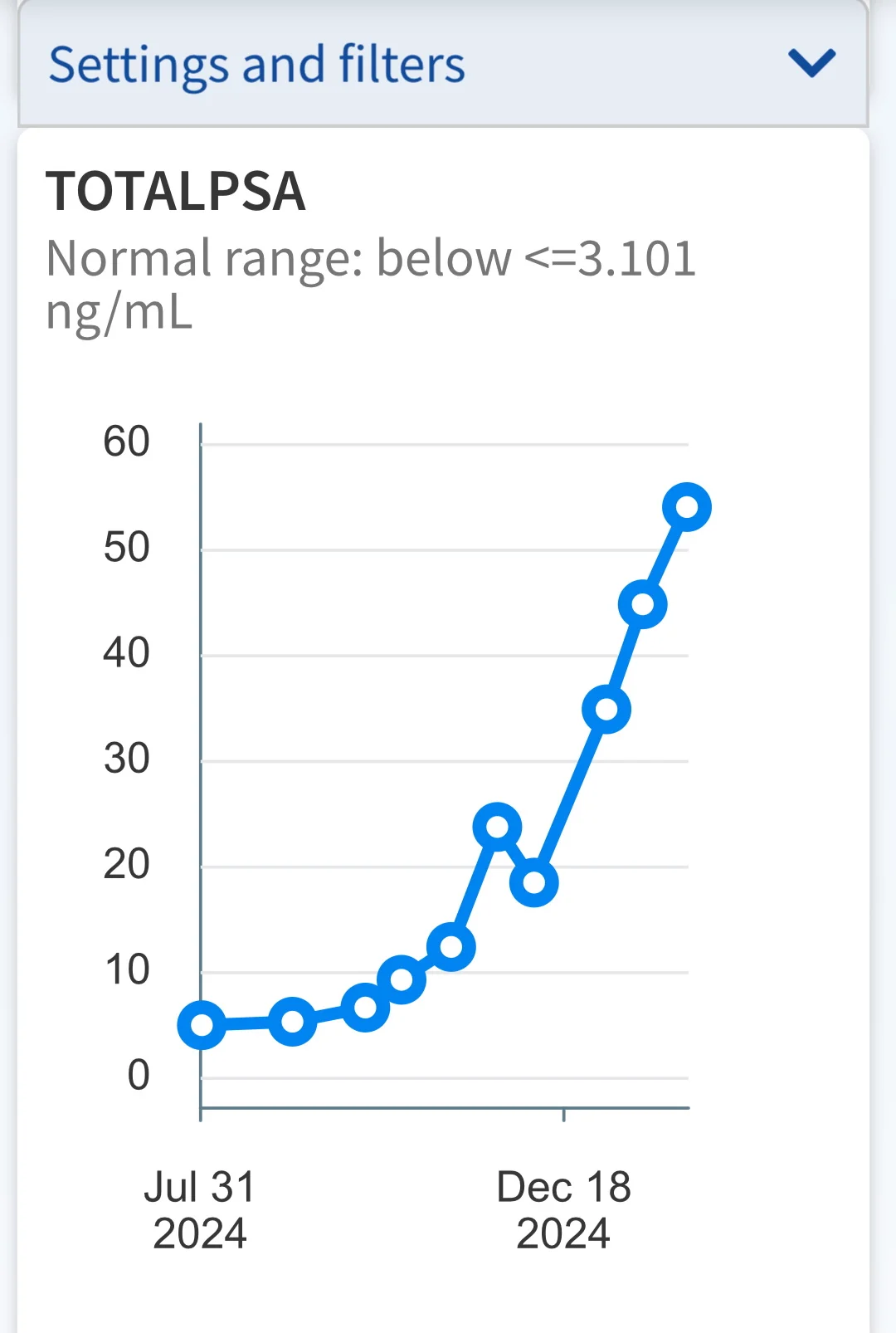
Update: PSA remained roughly 1.7 to 1.8 for last 4 months after Provenge but yesterday's 30-day PSA test revealed a jump to 3.190 so something is growing quick. I have been off of all ADT since finishing fourth LU-177 injection five months ago and one SBRT treatment 4 months ago.
After LU-177, PSA had been climbing quick until leveling off at 1.77 even as testosterone slowly returned.
New PSMA scan scheduled for next week but I have a feeling tumors won't show up.
What's next?

-
Hi,
Look at it this way, if your feeling good, and the PET scan is negative, is that such a bad thing? Unless you can find some cancer spots to treat, what else can you do. Sounds like the PET scan/PSA test could be the indicators on when to restart some form of treatment like Proton therapy or maybe Cryotherapy. Unfortunately it sounds like you have tried a lot of the traditional treatment protocols. If your still on them, I would stay off the TRT drugs. I don’t know what other types of treatment or test trials your doctor team could get you involved with. Good luck and keep up the fight……..
Dave 3+4
-
-
Thanks Dave. Unfortunately not all prostate cancer tumors are PSMA avid. That is they don’t show up on PSMA scans so sometimes it’s necessary to do a different kind of scan. Maybe FDG?
just because we haven’t seen it yet doesn’t mean that it doesn’t exist. I am somewhat alarmed that PSA doubled in the last 30 days.
-
Hi,
PET scans with Ga 68 PSMA-11, FDG tracers are very good at finding metastatic Pca from what I have read. Do you think it’s the size of the cancerous cell cluster that makes it undetectable? I would think even a PET scan would have certain limits on picking up very, very, small lesions. Might have to wait until the cell cluster grows large enough to be picked up by one of the tracers above. Wait and see game?
Dave 3+4
-






Discussion Boards
- All Discussion Boards
- 7 Cancer Survivors Network Information
- 6 Welcome to CSN
- 1 CSN Update
- 122.7K Cancer specific
- 2.8K Anal Cancer
- 457 Bladder Cancer
- 311 Bone Cancers
- 1.7K Brain Cancer
- 28.6K Breast Cancer
- 410 Childhood Cancers
- 28K Colorectal Cancer
- 4.6K Esophageal Cancer
- 1.2K Gynecological Cancers (other than ovarian and uterine)
- 13.1K Head and Neck Cancer
- 6.4K Kidney Cancer
- 682 Leukemia
- 805 Liver Cancer
- 4.2K Lung Cancer
- 5.1K Lymphoma (Hodgkin and Non-Hodgkin)
- 243 Multiple Myeloma
- 7.2K Ovarian Cancer
- 71 Pancreatic Cancer
- 494 Peritoneal Cancer
- 5.7K Prostate Cancer
- 1.2K Rare and Other Cancers
- 545 Sarcoma
- 745 Skin Cancer
- 663 Stomach Cancer
- 194 Testicular Cancer
- 1.5K Thyroid Cancer
- 5.9K Uterine/Endometrial Cancer
- 6.5K Lifestyle Discussion Boards