The Cancer Survivors Network (CSN) is a peer support community for cancer patients, survivors, caregivers, families, and friends! CSN is a safe place to connect with others who share your interests and experiences.
lump in neck

My husband had cancer diagnosed in march 2016 .He went through radiation and chemo and had surgery in July. All went well no spread of the cancer to borders. He is having a hard time eating. He had a dialation last month and is having another next week. He clams he feels a lump or something in his upper throat that is where he feels things get stuck and he throws up often right after eating. He has had scopes and swallow test that do not show anthing wrong. Has anyone else had this feeling and what did you do to fix it. Thanks for any help you can offer.
Comments
-
I have swallowing issues occationally
I had surgery about six and a half years ago, and I still have some difficulty with swallowing. Particularly, if I eat too quickly, or do not take time to chew very thoroughly.
I have found that some foods do give me more difficulty than others. Bread is one that causes issues along with some meats that can be stringy like chicken or some fish. I also have issues with things like rice. I have to take periodic sips of liquid to make things go down as I am eating.
If your husband has had endoscopies and they do not show any issues you might consider seeing an ENT doctor to see if there are any mechanical swallowing issues.
Best Regards,
Paul Adams
McCormick, South Carolina
DX 10/2009 T2N1M0 Stage IIB - Ivor Lewis Surgery 12/3/2009
Post Surgery Chemotherapy 2/2009 – 6/2009 Cisplatin, Epirubicin, 5 FU
Six Year Survivor -
ent
My husband saw a ent he looked down with a light and saw nothing out of the ordinary. He had a swallow test done and it showed something getting stuck in the esophgaus. His surgeon keeps saying it was not very constricted. He is going to do anothe dialation and is going to use a balloon from the esopgaus into the stomach. He did not do this the last time. My husband feel food is getting caught at the back of the throat. They keep saying nothing is there but he keeps throwing up most of what he eats. I hope tomorrow procdure helps . Thanks for the help it helps to know that he is not the only one with these problems.
-
Mink~A balloon dilation will probably solve the problem
Hello Mink:
Your husband might be experiencing what is a common occurrence with EC patients after an Esophagectomy. My husband started clearing his throat and felt like there was saliva that he needed to swallow. This occurred two weeks after his discharge. So the next visit, he mentioned it to Dr. Luketich @ UPMC. Dr. Luketich said this was common among many EC patients. He explained that a small ridge of scar tissue can form a tiny ring around the anastomosis (place where organs are rejoined.) Either saliva or a tiny speck of food can rest on that ledge instead of going straight down. Now you know the “muscular” action of the old Esophagus is not there, and the food goes down in a different way. It also lends itself to stomach acid working its way back up the new gastric tube because there is no longer a sphincter that once separated the stomach from the Esophagus. And that by the way is where most Esophageal Cancers are now occurring. Adenocarcinoma at the GastroEsophageal junction. Now that is why your husband must sleep elevated to keep the acid working its way right back up to the throat. That’s why nothing should be eaten 3 hours prior to bedtime, and of course one should not lie down right after eating. Moreover, it’s suggested that drinking of liquids should be in between the many “mini” meals that he will be eating during the day. And of course, the consistency of those foods will play a part in how the food proceeds down the new tube.
Now since your husband had his surgery in March of 2016, his eating patterns are still in flux. It took my husband 9 months before he stopped the weight loss, and maintained a steady weight. He was overweight (fat before political correctness set in) at 6 ft. and 275. He lost 60 # during the first 9 months. Then it leveled out. Now he is putting weight back on and I’ve sworn I’m not buying anything bigger than a size 40 waist. Of course, I could threaten not to cook, but I’m a good cook and we love to eat. But he doesn’t eat two plates full as he once did. However, his only symptom was a hiccup right when he took the first bite of food. He did not smoke or consume alcohol (two things highly suspect for EC) however, a multitude of patients still get this cancer. Usually difficulty swallowing or acid reflux or heartburn are the causes, but patients somehow adjust their eating habits until symptoms can no longer be ignored. Furthermore, I fault doctors who do not recommend their patients undergo an Endoscopy. Sadly, for many it is too late, and Stage IV is the diagnosis. My husband was nearing that stage at Stage III with 2 affected local lymph nodes. (T3N1M0)
So I would think that a balloon dilation would have been the first normal course of action, but according to the video and comments below, some doctors do not always perform the balloon dilation. Now although this article is written to explain the methods of dilation, it is also performed on people who have never had an Esophagectomy, but still have difficulty swallowing. Both my sister and my brother have had multiple dilations during their lifetime although neither of them were ever diagnosed with Esophageal Cancer. But in your husband’s case, it could well be the result of the healing process of the anastomosis. And that area is very tender, and a doctor has to be very careful not to cause a perforation. That is a possibility but is not usually the case.
My husband had two of these balloon dilations in the first 6 months, and have needed none since then. So I hope this is the cause of your husband’s regurgitation problems. The common symptom of feeling like something is stuck in the throat is often how patients describe their problem. Usually, a balloon dilation is all that is needed, and I hope that is all your husband requires. My husband had no ill effects, and the most he might have experienced would be a sore throat but that did not even occur. But you’re certainly right to be wondering what’s going on. Hope this procedure later today takes care of the problem.
All the best,
Loretta - Wife of William, EC Stage III, who underwent an Ivor Lewis Minimally Invasive Esophagectomy at the University of Pittsburgh Med. Ctr. On May 17, 2003 (first diagnosed in Nov. of 2012 and is now entering his 14th yr. of clean scans. Thank God.
________________________________________________________
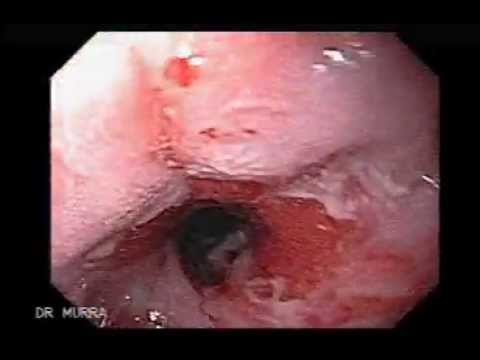
“Esophageal Dilation due to a narrowing of the esophagus
Dr.Julio Murra Saca Endoscopia El Salvador - Uploaded on Apr 15, 2007
What is Esophageal Dilation? Esophageal dilation is a procedure that allows your doctor to dilate, or stretch, a narrowed area of your esophagus [swallowing tube]. Doctors can use various techniques for this procedure. Your doctor might perform the procedure as part of a sedated endoscopy. Alternatively, your doctor might apply a local anesthetic spray to the back of your throat and then pass a weighted dilator through your mouth and into your esophagus.
Why is it Done? The most common cause of narrowing of the esophagus, or stricture, is scarring of the esophagus from reflux of acid occurring in patients with heartburn. Patients with a narrowed portion of the esophagus often have trouble swallowing; food feels like it is "stuck" in the chest region, causing discomfort or pain.
Less common causes of esophageal narrowing are webs or rings (which are thin layers of excess tissue), cancer of the esophagus, scarring after radiation treatment or a disorder of the way the esophagus moves [motility disorder].
How Should I Prepare for the Procedure? An empty stomach allows for the best and safest examination, so you should have nothing to drink, including water, for at least six hours before the examination. Your doctor will tell you when to start fasting. Tell your doctor in advance about any medications you take, particularly aspirin products or anticoagulants (blood thinners). Most medications can be continued as usual, but you might need to adjust your usual dose before the examination. Your doctor will give you specific guidance.
Tell your doctor if you have any allergies to medications as well as medical conditions such as heart or lung disease. Also, tell your doctor if you require antibiotics prior to dental procedures, because you might need antibiotics prior to esophageal dilation as well.
What Can I Expect during Esophageal Dilation? Your doctor might perform esophageal dilation with sedation along with an upper endoscopy. Your doctor may spray your throat with a local anesthetic spray, and then give you sedatives to help you relax. Your doctor then will pass the endoscope through your mouth and into the esophagus, stomach and duodenum. The endoscope does not interfere with your breathing. At this point your doctor will determine whether to use a dilating balloon or plastic dilators over a guiding wire to stretch your esophagus.
You might experience mild pressure in the back of your throat or in your chest during the procedure. Alternatively, your doctor might start by spraying your throat with a local anesthetic. Your doctor will then pass a tapered dilating instrument through your mouth and guide it into the esophagus.
What Can I Expect after Esophageal Dilation? After the dilation is done, you will probably be observed for a short period of time and then allowed to return to your normal activities. You may resume drinking when the anesthetic no longer causes numbness to your throat, unless your doctor instructs you otherwise. Most patients experience no symptoms after this procedure and can resume eating the next day, but you might experience a mild sore throat for the remainder of the day. If you received sedatives, you probably will be monitored in a recovery area until you are ready to leave. You will not be allowed to drive after the procedure even though you might not feel tired. You should arrange for someone to accompany you home, because the sedatives might affect your judgment and reflexes for the rest of the day.
What are the Potential Complications of Esophageal Dilation? Although complications can occur even when the procedure is performed correctly, they are rare when performed by doctors who are specially trained. A perforation, or hole, of the esophagus lining occurs in a small percentage of cases and may require surgery. A tear of the esophagus lining may occur and bleeding may result. Complications from heart or lung diseases are potential risks if sedatives were used. Symptoms of this disorder vary and may include difficulty swallowing (dysphagia), painful swallowing, regurgitation of food and weight loss. Further complications may also arise if the stricture is left untreated. Fortunately, esophageal dilation offers potential relief and healing for those suffering from esophageal stricture, Dr. Julio Murra Saca perform a dilation with hydrostatic Balloon. www.murrasaca.com
____________________End _______________________


 https://www.youtube.com/watch?v=UPlMtKpld78
https://www.youtube.com/watch?v=UPlMtKpld78Discussion Boards
- All Discussion Boards
- 7 Cancer Survivors Network Information
- 6 Welcome to CSN
- 1 CSN Update
- 122.7K Cancer specific
- 2.8K Anal Cancer
- 457 Bladder Cancer
- 311 Bone Cancers
- 1.7K Brain Cancer
- 28.6K Breast Cancer
- 410 Childhood Cancers
- 28K Colorectal Cancer
- 4.6K Esophageal Cancer
- 1.2K Gynecological Cancers (other than ovarian and uterine)
- 13.1K Head and Neck Cancer
- 6.4K Kidney Cancer
- 682 Leukemia
- 805 Liver Cancer
- 4.2K Lung Cancer
- 5.1K Lymphoma (Hodgkin and Non-Hodgkin)
- 243 Multiple Myeloma
- 7.2K Ovarian Cancer
- 71 Pancreatic Cancer
- 493 Peritoneal Cancer
- 5.7K Prostate Cancer
- 1.2K Rare and Other Cancers
- 544 Sarcoma
- 745 Skin Cancer
- 663 Stomach Cancer
- 194 Testicular Cancer
- 1.5K Thyroid Cancer
- 5.9K Uterine/Endometrial Cancer
- 6.5K Lifestyle Discussion Boards